EHDS implementation will not fail because of regulation or standards. It will fail if governance, semantic quality, and delivery capacity do not keep pace with ambition.
Across Europe, health systems are now making infrastructure decisions that will shape how clinical data moves, persists, and retains meaning for the next decade. While the EHDS regulation defines a common direction for interoperability and data sharing, stakeholder interviews across Europe reveal a more operational reality beneath it: the decisive barriers are rarely the standards themselves. The real pressure points are fragmented governance, inconsistent semantic quality, legacy infrastructure, and limited implementation capacity. As one stakeholder in our recent research on EHDS readiness put it, “the challenge is no longer understanding where Europe wants to go. It is whether health systems are structurally prepared to get there.”
1. Three starting points, three realistic timelines
While the strategic ambition behind EHDS is broadly shared across Europe, operational readiness is not. Stakeholder interviews surfaced three distinct implementation realities depending on the maturity of the environment.
High maturity
Compliance by 2029 realistic · usability +2-3 yrs
- Operational shared care records in active use
- Routine structured data capture with terminology services
- Modular, API-driven architectures
- Clear governance, substantial in-house capacity
EHDS is the next logical step.
Medium maturity
4-6 years for meaningful implementation
- Structural infrastructure with incomplete coverage
- Mixed semantic readiness, persistent free text
- Hybrid modern-legacy architectures
- Defined but capacity-constrained governance
Substantial but achievable effort.
Lower maturity
7-10 years including foundational work
- Manual exchange processes
- Predominantly narrative clinical documentation
- Legacy vendor lock-in
- Fragmented governance and limited implementation capacity
Foundational capabilities required first.
“For some countries this is the next step. For others, it feels like being asked to run before you’ve learned to walk.” — Stakeholder interview
Categories are deliberately broad. Most countries sit between them and the timelines should be read as directional rather than absolute. The difference between these groups is not simply technical sophistication but institutional maturity: the ability to govern health data consistently across fragmented systems, align national priorities, and sustain long-term transformation capacity.
That is why EHDS readiness cannot be reduced to a compliance checklist. Two countries may appear similarly advanced on paper while facing completely different operational realities underneath.
2. EHDS readiness requirements: four structural conditions
Four structural conditions separate regulatory alignment from operational value.
1. Coherent data architecture: what EHDS mandates, and what implementation actually requires
One of the clearest themes across stakeholder interviews was not disagreement about standards, but growing clarity about architectural roles.
FHIR solves one problem exceptionally well: exchange. But exchange alone does not guarantee continuity of meaning once data reaches another system. That responsibility sits deeper in the stack, inside the clinical models, terminology governance, and persistence layers that determine whether information remains interpretable over time.
“FHIR is excellent for exchange, but if you don’t have a strong semantic backbone underneath, you just move inconsistency faster.” — Senior health IT architect
EHDS mandates the European Electronic Health Record exchange Format (EEHRxF), built on HL7 FHIR, for cross-border exchange of priority data categories like Patient Summaries and ePrescriptions. But the architecture beneath EEHRxF is what determines whether implementations succeed.
The emerging consensus points to a layered approach: openEHR or equivalent clinical modelling frameworks to define and govern meaning at rest, FHIR-based APIs to move and access data across systems, controlled terminologies (SNOMED CT, LOINC, ICD) to ensure consistent coding, and implementation guides to ensure uniform interpretation across borders.
Implementations that succeed will be the ones that treat persistence, exchange, and semantics as separate challenges requiring different tools and governance models, then connect them deliberately. Two hospitals may both claim to exchange a “patient summary”, while one encodes diagnoses using SNOMED CT and the other relies heavily on free text. Technically, both systems may comply. Clinically, the receiving clinician experiences something entirely different.
Semantic quality is not an enhancement layered on top of EHDS implementation. It is the condition that determines whether EHDS delivers meaningful value at all.
2. Governance clarity and accountability
Technology does not implement itself. Sustainable EHDS execution depends on clear ownership structures, aligned responsibilities, and long-term operational accountability.
“Technology is not the bottleneck. It’s governance that will determine whether EHDS succeeds or stalls.” — National eHealth coordinator
Stakeholders repeatedly highlighted the risks of fragmented governance, particularly in systems where national coordination mechanisms remain weak or responsibilities overlap between institutions. Many interviewees also pointed toward national aggregation models as a practical way to reduce implementation complexity. Rather than requiring every individual healthcare organisation to connect independently at European level, national or regional interoperability hubs can centralise governance, simplify coordination, and reduce operational fragmentation.
EHDS implementation will ultimately depend less on temporary programme structures and more on whether durable governance mechanisms exist beyond individual projects or funding cycles.
3. Clinical usability and workflow integration
Interoperability only creates value when it works inside real clinical workflows.
This becomes most visible in structured data capture. Across many healthcare systems, clinicians still rely heavily on narrative documentation because it remains faster and more flexible in daily practice. But free text creates significant limitations for interoperability, longitudinal care, analytics, and secondary use.
“You can’t share what you don’t have and you can’t interpret what’s locked in free text.” — Standards expert
The challenge is not simply increasing structure. It is doing so without creating additional administrative burden for clinicians already operating under pressure.
The European Patient Summary will likely become the first large-scale operational test of this balance. If clinicians encounter incomplete, poorly coded, or difficult-to-use information, confidence in broader EHDS ambitions may erode quickly.
4. Public trust and transparency
EHDS expands both the availability of health data and the responsibility attached to it.
Trust is not a communications exercise layered onto implementation afterwards. It is a structural requirement built into the architecture, governance, and operational design of the system itself. Patients need to understand who accesses their data, why it is accessed, and what safeguards exist around it. Transparent governance, auditability, and visible accountability mechanisms are essential if EHDS is to maintain long-term legitimacy across Member States.
Because trust is difficult to rebuild once lost, implementation decisions made today need to account not only for technical feasibility, but also for public perception and institutional credibility.
These four conditions are the foundations upon which successful EHDS implementation rests.
Data architecture
Separate persistence, exchange, and semantics. FHIR moves data, openEHR preserves meaning at rest. Terminology governance connects both layers consistently over time.
Governance
Long-term accountability, not project ownership. National coordination models reduce fragmentation, clarify responsibility, and support sustainable implementation over time.
Clinical usability
Structured data must work in practice. EHDS depends on structured capture at source without creating additional burden for clinicians or disrupting care delivery.
Trust & transparency
Trust must be operational, not assumed. Clear access rules, auditability, and visible safeguards are essential for public confidence in EHDS.
Remove any one foundation and EHDS implementation falters.
3. What is the EHDS implementation timeline?
While many EHDS discussions still feel theoretical, the regulatory timeline is already moving.
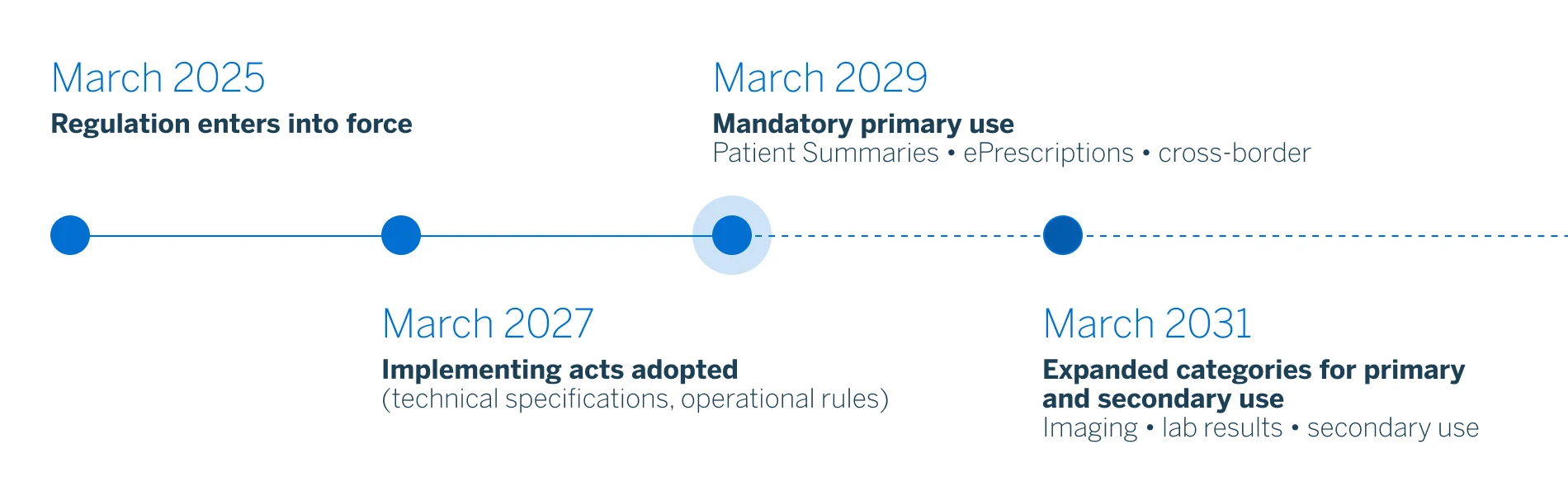
The EHDS regulation entered into force on 26 March 2025, with implementation unfolding through a phased sequence over the coming years:
- March 2027: adoption of key implementing acts defining technical specifications and operational requirements.
- March 2029: mandatory application of primary use provisions, including cross-border exchange of Patient Summaries and ePrescriptions.
- March 2031: expansion to additional data categories such as medical imagery, laboratory results, and discharge reports, alongside broader secondary use obligations.
Enforcement is not symbolic. Organisations and vendors that fail to comply, block data sharing, or misuse the system can face GDPR-style penalties: fines of up to 20 million euros or 4% of global annual turnover, plus the possibility of temporary suspension from the European Health Data Space itself.
The milestones above establish the regulatory baseline, but operational readiness depends heavily on national digital maturity. Semantic harmonisation, modular architecture design, governance clarification, and workflow redesign cannot realistically be compressed into the final years before 2029. For digitally mature systems, the timeline represents acceleration, but for fragmented systems, it represents a race against accumulated structural debt.
4. Avoiding compliance theatre
EHDS implementation can be approached in two ways. The first will meet the regulatory deadlines on paper. The European Electronic Health Record exchange Format will be deployed, conformance tests will pass, the compliance reports will be filed. But the underlying data will remain fragmented, free text will still dominate clinical documentation, and the cross-border exchange will move information that no receiving system can meaningfully use. This is compliance theatre.
The second kind of implementation will use the same regulatory pressure to drive durable reform: stronger data quality and terminology governance, clearer institutional ownership, modular and vendor-neutral architectures, and consent and identity infrastructure that holds under scale. These investments create value regardless of how EHDS itself evolves. They turn the regulation from a deadline into a capability dividend.
The years leading to 2029 are a narrow window for the second kind. Whether EHDS becomes a catalyst for durable digital health transformation or an additional administrative layer will depend less on implementing acts and more on the structural decisions taken now.
To explore how healthcare leaders across Europe are approaching those decisions, including readiness gaps, architectural priorities, governance challenges, and no-regret investments already shaping national strategies, access the full EHDS implementation readiness research.
FAQ
When does EHDS become mandatory?
EHDS becomes mandatory in stages, with major obligations beginning from 2029. The regulation entered into force in March 2025, but implementation follows a phased timeline. Key implementing acts are expected in 2027, while mandatory primary use obligations, including cross-border patient summaries and ePrescriptions, begin from 2029. Additional data categories, such as imaging, laboratory results, and discharge reports, expand from 2031. For health systems, this means EHDS preparation needs to start well before the legal deadlines.
What are the penalties for EHDS non-compliance?
EHDS non-compliance can lead to GDPR-style penalties, including fines of up to €20 million or 4% of global annual turnover. Organisations and vendors that fail to comply, block data sharing, or misuse the system may also face temporary suspension from the European Health Data Space. Beyond legal penalties, non-compliance creates operational risks: rushed implementation, procurement pressure, weaker interoperability, and reduced ability to participate in cross-border health data exchange. Enforcement is therefore not symbolic; EHDS creates both regulatory and strategic consequences.
How should health systems prepare for EHDS implementation?
Health systems should prepare for EHDS by building operational capability, not just checking compliance requirements. The most important preparations include improving structured clinical data capture, strengthening terminology governance, clarifying ownership, investing in modular and vendor-neutral architecture, and ensuring identity, consent, auditability, and access rules are ready for scale. Because digital maturity varies widely across Europe, preparation timelines will differ. The safest approach is to prioritise no-regret investments that create value regardless of how technical specifications evolve.
Are European health systems ready for EHDS?
European health systems are not equally ready for EHDS, and readiness varies significantly by digital maturity. Some countries already have shared care records, structured data capture, governance models, and interoperability infrastructure in place. Others still depend on fragmented systems, manual exchange, free-text documentation, and legacy vendor environments. This means EHDS implementation will not follow one uniform timeline. For mature systems, EHDS may be an acceleration. For fragmented systems, it is a race against structural debt.